Definition
Cerebral hemorrhage is a type of intracranial bleeding when the blood leaves the damaged blood vessel and distributes in different areas of the brain. Many times such bleeding is a consequence of brain trauma although it may occur spontaneously as well (non-traumatic intracerebral bleeding).
It is essential to differentiate the bleeding in the very brain from bleeding that also occurs inside the skull but remains localized outside the brain tissue. Namely, epidural, subdural as well as subarachnoid bleeding are all associated with hemorrhage inside the skull. The blood that has left the damaged blood vessel in this case, however, remains outside the brain. Intracerebral bleeding, on the other side, is the one associated with blood accumulation inside the brain. It can be further classified into intraparenchymal and intraventricular hemorrhage. The former refers to blood collection located between the brain cells and outside the ventricular system of the brain while the latter is actually bleeding in the ventricles of the brain.
As for symptoms and signs of cerebral bleeding, they basically depend on the area of the brain affected by the bleed and the functions it is in charge with. Also, apart from specific symptoms and signs there are general signs of cerebral bleeding triggered by an increase in intracranial pressure due to uncontrollable or excessive bleeding. These include sudden and severe headache accompanied by nausea and vomiting as well as additional neurological signs like steady development of neurological losses (e.g. weakness, inability to move, numbness, speech difficulty, vision loss etc.), seizures and loss of consciousness.
Diagnosis
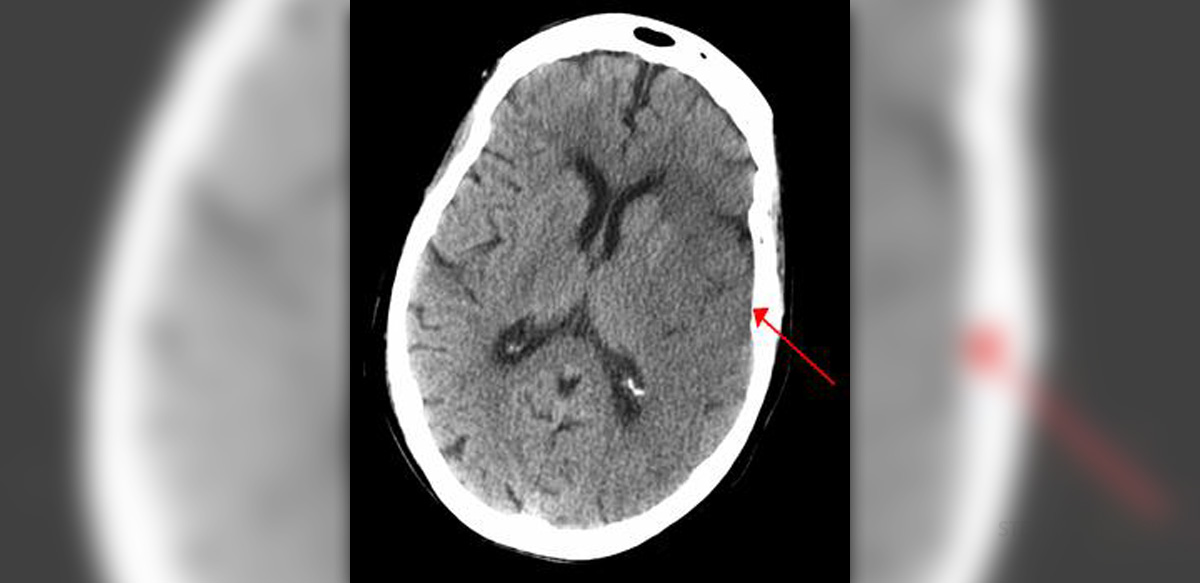
A well experienced doctor may suspect cerebral bleeding after taking patient's history and performing a neurological exam. However, in order for him/her to confirm the diagnosis and identify the source of bleeding, patients must undergo CT scan of the brain. CT scan is sensitive enough to reveal bleeding and allows suitable insight in the amount of brain tissue affected.
Cerebral hemorrhage is always an emergency so the diagnosis must be established quickly and treatment should start even before the diagnosis is definitely confirmed by CT scan.
In case CT scan of the brain does not show any signs of bleeding, the patient undergoes spinal tap. This test will confirm or rule out subarachnoid hemorrhage, the condition that may resemble intracerebral bleeding. Sometimes doctors additionally perform CT angiogram.
Finally, even if the diagnosis is confirmed on time and a patient treated instantly, the bleeding may cause serious and long-term complications some of which are swallowing difficulties, memory/thinking/talking/comprehension/writing/reading issues, changes in vision, paralysis of different degree, personality changes and loss of consciousness/coma.
Management
There are several treatment options for cerebral hemorrhage. It is essential to start with treatment as soon as possible, stop further bleeding and prevent permanent damage to the affected parts of the brain.
In case bleeding is associated with hypertension (which is often the case) patients are administered antihypertensives. The goal is to maintain blood pressure at 110 mmHg. Furthermore, the bleeding may be limited if one receives factor VIIa within 4 hours after the bleeding has begun. This factor also accelerates the formation of a blood clot preventing further blood loss but it may cause problems by triggering thromboembolism in susceptible individuals.
Diuretics and/or corticosteroids are administered to reduce the increased intracranial pressure, hyperthermia is dealt with acetaminophen while coagulopathies are brought under control with the assistance of frozen plasma and vitamin K. Seizures require antiepileptic drugs. Stress peptic ulcers may be successfully prevented with H2 antagonists.
Surgery is performed only in limited number of patients. Sometimes it is simple not possible to reach certain parts of the brain and stop the bleeding without damaging the nearby structures. There are several surgeries that may stop the bleeding. Sometimes doctors insert a catheter into the brain and close or dilate blood vessels. Basal ganglia hemorrhage can be treated by stereotactic surgery and endoscopic drainage. Still, certain patents require more invasive surgical approach.
Supportive measures include tracheal intubation, assisted ventilation (unconscious patients and those with airway obstruction) and intravenous fluids that maintain optimal level of all the electrolytes in the body.
Once the bleeding is stopped and patients start to feel better, they are engaged in physical therapy. Physical therapy is especially beneficial for all those with neurological sequelae such as paralysis or swallowing issues. Occupational therapy may be recommended as well.
Relevant Data
It is estimated that approximately 40% of all patients suffering from cerebral bleeding die due to the very bleeding or the associated complications.
When it comes to spontaneous cerebral bleeding 34-50% of patients die within 30 days and almost a half of all patients do not survive more than 2 days.
In the United States 20% of people suffering from cerebrovascular disease are actually affected by cerebral hemorrhage. The condition is reported more in patients of African ancestry.
Fortunately, by preventing atherosclerosis and timely treating hypertension, the majority of cases of cerebral hemorrhage can be successfully prevented.
Your thoughts on this
Loading...