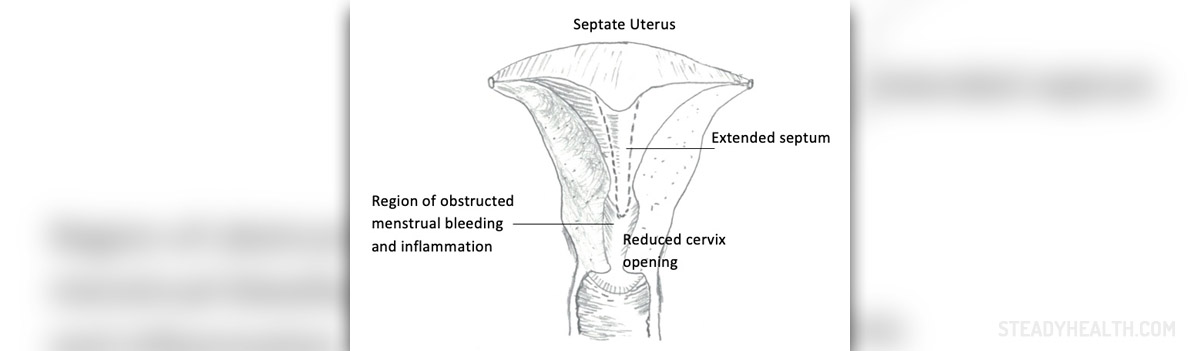
Septate Uterus
Septate uterus represents the most common müllerian anomaly. In this condition, the uterus is divided by a fibrous septum and instead of one cavity, there are two cavities inside the uterus. The septum may extend to the internal opening of the cervix and this is known as a complete septum. On the other hand, the membrane may not extend completely to the internal opening of the cervix. This septum is known as the partial septum.
Septate uterus develops as a mistake in intrauterine development of the uterus. The exact cause of this anomaly has not been identified yet.
Consequence of Septate Uterus
The presence of the septum does not interfere in the process of fertilization and implantation of the egg. However, it can interfere in the course of pregnancy. Septate uterus may be a cause of miscarriage or can be related to certain complications during pregnancy. Women who have septate uterus usually face early miscarriage. This can be easily explained by the fact that the blood-starved median septum is covered by endometrium of lower quality comparing to that of the blood-rich sidewalls. It may occur that the egg is implanted into the septum and lack of nourishment is what leads to early miscarriage. Apart from early and late miscarriage, the septate uterus may cause premature labor, premature birth, intrauterine growth retardation, and fetal malpresentation at birth.
Diagnosis of Septate Uterus
In case, there is not a vaginal septum or double cervix the gynecologist simply cannot diagnose the condition during gynecological examination. The condition may stay undiagnosed until the woman experiences repeated miscarriages. The perfect method for setting the diagnosis of the septate uterus is a hysterosalpingogram. This examination includes the injection of a dye into the uterus and taking an X-ray of the uterus and accompanying reproductive organs. Septate uterus may be also visualized with ultrasound, MRI and hysteroscopy.
Surgery for Septate Uterus
This medical condition can be easily treated by a simple surgical procedure. After the surgery the woman is able to conceive and give birth to full-term baby without any fear of repeated miscarriages caused by the septum.
Metroplasty is a surgery performed in women suffering from the septate uterus. This surgery used to be performed through an abdominal incision. Now there is hysteroscopic metroplasty which is less invasive comparing to abdominal approach. Metroplasty is performed in women who have suffered from recurrent abortions. The goal of the surgery is removal of the septum. This is a very successful surgery and up to 80% manage to carry a baby to term.
Over the years, numerous classification systems have been proposed to classify female genital anomalies. According to the European Society of Human Reproduction and Embryology–European Society for Gynaecological Endoscopy classification system, any uterus with a normal outline and an internal fundal midline indentation exceeding 50% of the uterine wall thickness is defined as septate. A complete septate uterus is further characterized by full division of the uterine cavity up to the level of the internal cervical os. Although the septum is usually restricted to the uterine corpus, it may also extend through the cervix and vagina, potentially leading to infertility and miscarriage.
- Traditionally, a septate uterus is diagnosed by laparoscopy and hysteroscopy, and hysteroscopic metroplasty is considered the first-line therapy for restoring the uterine cavity, with high levels of improvement to subsequent reproductive outcomes. However, there is still uncertainty of the effectiveness of resecting the uterine septum because the evidence is mainly based on retrospective studies. Unfortunately, data of prospective studies are extremely limited.
- The study population comprised 92 women with complete septate uteri. Hysteroscopic metroplasty and laparoscopy were performed simultaneously in these patients. The postoperative reproductive outcome of each patient was evaluated.
- In the primary infertility group, there were 32 (40%) pregnancies. In the abortion group, the number of miscarriages decreased from 68 (94.44%) to 5 (10.42%), while the number of live births increased from 1 (1.39%) to 42 (87.50%) after resection compared with before resection.
- The cumulative probability of pregnancy and that of live-birth pregnancy in the abortion group were significantly higher than those in the primary infertility group after surgery.
- Furthermore, resection of the cervical septum resulted in a significantly higher cumulative probability of live birth compared with preservation of the cervical septum.
- Another interesting finding in our study is that subsequent pregnancy-related uterine rupture and cervical cerclage were not observed in either group. Additionally, the incidence of cesarean delivery was significantly higher when the cervical septum was preserved. Cervical dystocia resulting from a persistent cervical septum may be the main reason for this finding because we excluded social factors associated with cesarean sections. An increase in the caesarean section rate will inevitably increase maternal and infant complications. Therefore, resection of the cervical septum is of certain significance in clinical practice.
Your thoughts on this
Loading...