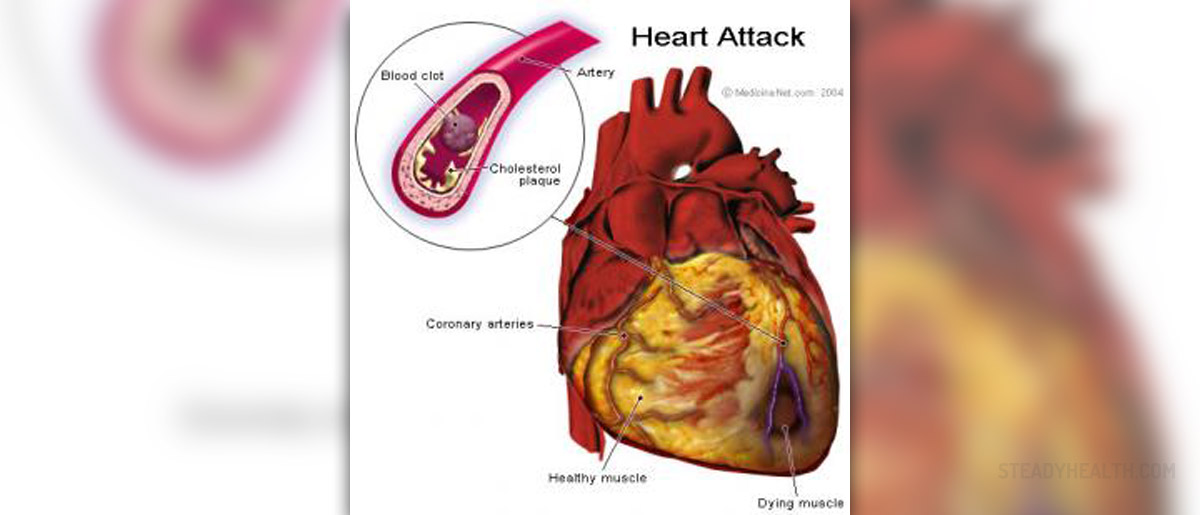
Acute myocardial infection (AMI) has a number of complications associated with it. Those include the following:
A failure of reperfusion, although less likely with the introduction of PCI (primary percutaneous coronary intervention), is only reduced by around 50%. Thus, it is still possible.
Infarct extension and post infarction angina appear in some patients, usually resulting in continuous or recurrent chest pains, protracted elevation of CK (creative kinas) level and new electro diagram changes. The diagnosis can be made with echocardiography or nuclear imaging. Medical therapy includes Aspirin, heparin, nitrates, and beta blockers use in patients suffering from myocardial infarction along with ongoing ischemic symptoms.
Reinfarction is more common in patients with previous myocardial infarction history. A recurrent infarction can be hard to diagnose within the first 2 days, so extra vigilance is advised.
Post infarction angina presents itself a couple of hours after AMI. It is most often found in patients with non-ST elevation myocardial infarction and those who have been treated with fibronolytics, instead of PCI.
Pulmonary edema can commonly appear after a myocardial infarction.Heart failure is usually caused by the amount of myocardial damage, by an arrhythmia or mitral regurgitation and ventricular sepal defect. The severity of the heart failure largely depends on the presence of any other complications.
Carcinogenic shock occurs in 5-20 percent of patients following myocardial infarction.The severity of cardiac failure is classified, for instance, with the Killip classification.
Carcinogenic I: no crackles and no 3rd heart sound Carcinogenic II: crackles in less than 50 percent of lung fields or a 3rd heart sound Carcinogenic III: crackles in over 50 percent of lung fields Carcinogenic IV: carcinogenic shockCardiac failure is often responsive to oxygen, diuretics and angiotensin-converting enzyme (ACE) inhibitors/angiotensin receptor antagonists.
Patients who show a left ventricular ejection fraction of 0.4 or less, along with diabetes or clinical signs of heart failure are to use an aldosterone antagonist such as eplerenone. This, however, should not be the case if contra-indicated by renal impairment or hyperkalaemia.
These are only some of the possible complications. Others include: ventricular sepal rupture and free wall rupture, acute mitral regurgitation, left ventricular aneurysm, right ventricular failure, left ventricular outflow tract obstruction. Also, a number of arrythmias may appear as a direct side effect. The following are most common: systolic, ventricular, bradycardia, senatorial dysfunction or heart block.
Thrombosis and embolic complications, pericarditis (very common) and Dressler’s syndrome are further examples. Depression is found in about 20 percent of patients following a myocardial infarction. The risk of mortality is significantly elevated due to this occurrence.
Your thoughts on this
Loading...