Lung Biopsy
Lung biopsy is a medical procedure that is performed in order to provide the specimen of the lung tissue. This lung tissue is further examined pathophysiologically and the doctor can set the definitive diagnosis of the disease.
This procedure is always performed if a doctor suspects lung tumors, tuberculosis or in case of some other abnormalities such as nodules whose etiology cannot be confirmed without pathohistological examination.
During bronchoscopy a doctor can take samples of the abnormal tissue and he/she can also perform certain maneuvers which will help a patient with symptoms of the disease.
After the Lung Biopsy
Depending on the approach the patients are given specific directions on how to behave to avoid possible complications.
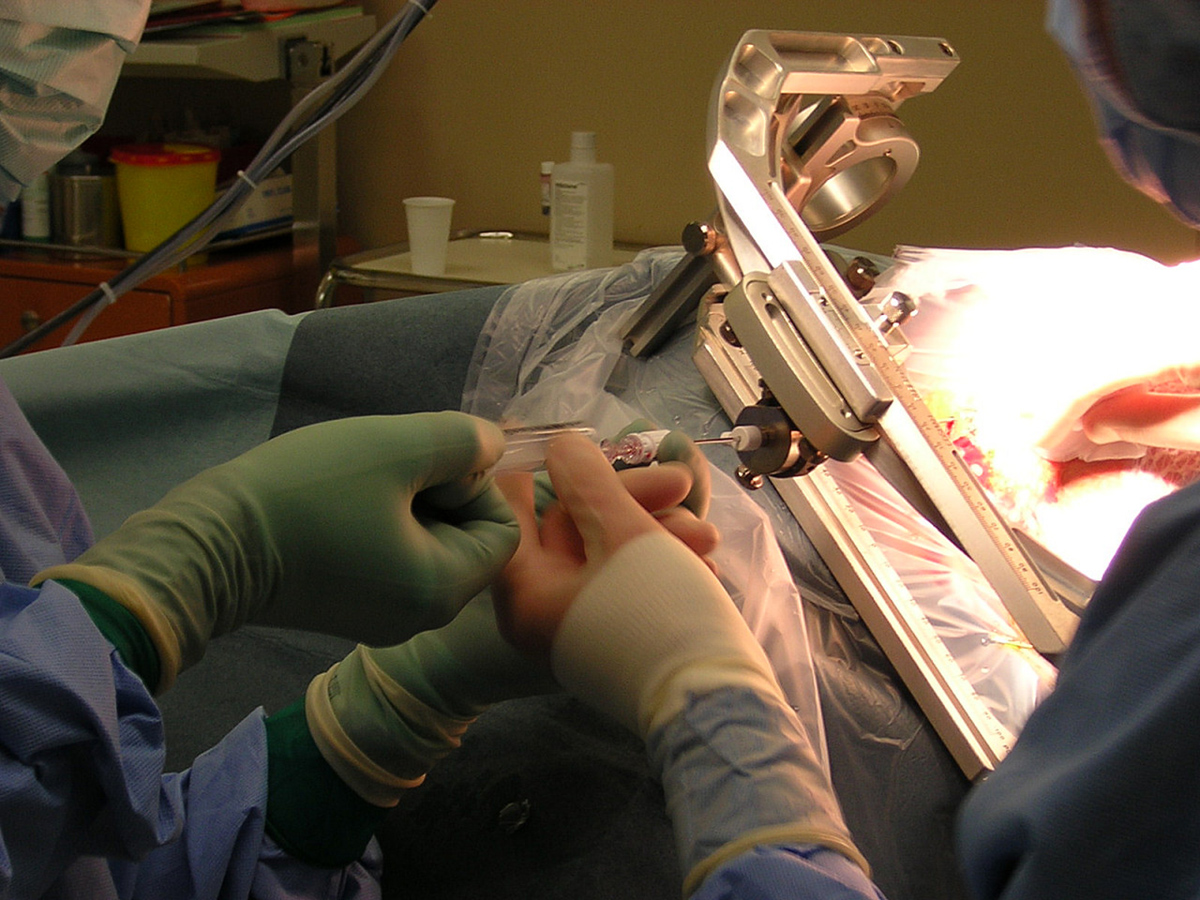
After the needle biopsy a patient is held to lie flat for a couple of hours. This prevents bleeding. The patient is released home and given additional advice on resuming normal activities. Bed rest should include two more days and then the patient can continue with regular daily activities. Strenuous activities including lifting heavy objects are strictly forbidden for a week.
After an open biopsy, VATS or mediastinoscopy patients stay in the hospital. They spend a certain time in the recovery room and then they are transferred to a hospital room. All the vital signs are closely monitored. Chest tubes need to stay in their place and they prevent the collapse of the lungs and assist in drainage of the blood and fluids. The tubes are removed after a day. Patients can complain about sore throat which is a consequence of endotracheal intubation or pain at the incision site. These are normal reactions brought under control by specific medications. The recovery time is longer than after the needle biopsy.
Complications of the Lung Biopsy
Prior to the biopsy a surgeon must be fully informed if patients are suffering from coagulopathies or take some medications since these can be risk factors for certain complications. Complications are also common in people who are suffering from other medical conditions.
Standard complications include bleeding, infections, and pneumonia. Pneumothorax is another complication that mostly occurs in open biopsies.
Bronchoscopic biopsy can cause spasms of the bronchial tubes and arrhythmia. Even infections such as pneumonia can occur.
After the needed biopsy the patient may cough up blood. This is a rather rare complication and affects only 5% of all patients. Additionally, patients can develop prolonged bleeding and infections.
In open biopsy infections and pneumothorax are the most common complications. Patients who had problems with breathing prior to the surgery are at higher risk of further breathing impairment after the surgery.
Mediastinoscopy does not commonly cause complications. Pneumothorax as well as prolonged bleeding are still possible. Even infections such as mediastinitis may occur. During a mediastinoscopy, some organs can be injured. They include the esophagus and larynx. In case the recurrent laryngeal nerve is damaged patients may develop chronic hoarseness.
- We performed a cross-sectional analysis of discharge records in four large, geographically diverse states in 2006. Our primary outcomes were risk of complications of CT-guided biopsy of a pulmonary nodule: the percent of biopsies complicated by hemorrhage, pneumothorax, or pneumothorax requiring chest tube.
- We used the 2006 Healthcare Cost and Utilization Project State Inpatient Databases and State Ambulatory Surgery Databases from the largest participating state in each census region (California, Florida, Michigan, New York). These states had a combined estimated adult population of 63,340,236, representing 28.2% of the 2006 United States (US) population.
- We calculated the overall rate of CT-guided lung biopsies per 100,000 adults in the selected states, and also age-standardized each state’s rate using the 2006 estimated US adult population.
- Of 22,176 CT-guided lung biopsies in the 4 states, 15,865 met our criteria of a single biopsy of a pulmonary nodule. There were statistically significant differences among states in patient, visit, and hospital characteristics.
- Characteristics associated with complications - age (60-69 years, versus age
Your thoughts on this
Loading...