Central serous retinopathy is an exudative chorioretinopathy. It features with an exudative neurosensory retinal detachment with or without associated retinal pigment epithelium detachment. The condition eventually leads to metamorphopsia and micropsia.
Central serous retinopathy generally occurs in people between the age of 20 and 50. It is more frequent among men (6:1). The condition has been connected with stress and stress hormones such as corticosteroids and epinephrine. It has been proven that people exposed to exogenous corticosteroids (for example people suffering from asthma, autoimmune disorders, certain skin conditions etc.) or people with increased level of endogenous corticosteroids (Cushing syndrome) or epinephrine are at higher risk for central serous retinopathy.
What Causes Central Serous Retinopathy?
There are several hypothesis regarding the actual cause of central serous retinopathy. They are based on epidemiologic and angiographic observations.
People suffering from central serous retinopathy show increased susceptibility to choroidal and RPE hyperpermeability with corticosteroids and epinephrine. Some disturbances in autonomic function may be responsible for spasm in the choroidal circulation. Choroidal Vasoconstriction due to epinephrine and corticosteroids is a potential cause of choroidal ischemia and hypermeability. Exctravasation of plasma proteins increases oncotic pressure in the extravascular space and this promotes malfunctioning of the RPE pump mechanism and causes an RPE leak. The final effect is neurosensory retinal detachment.
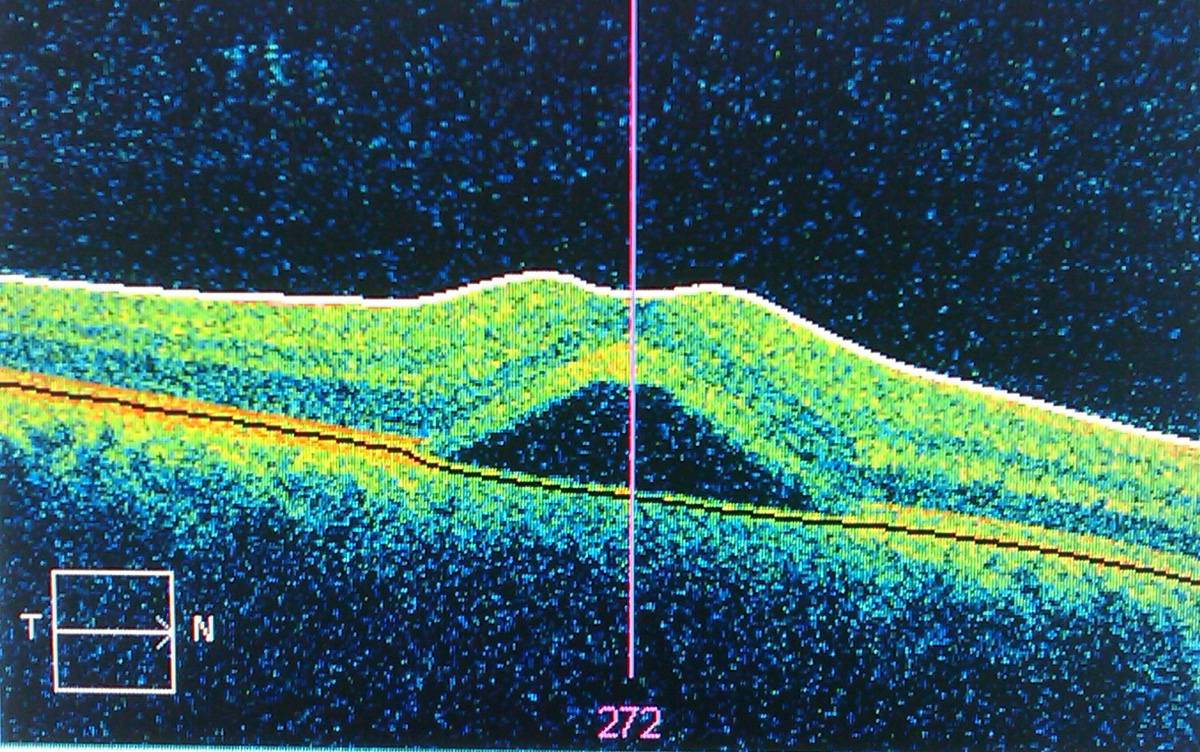
Clinical Characteristics of Central Serous Retinopathy
Patients suffering from central serous retinopathy develop central scotoma, metamorphopsia and micropsia. Visual acuity may be improved with small hyperopic correction. There is an evident reduction in contrast sensitivity and color saturation as well as increase in macular photostress recovery time. In case of serious retinal detachment there are subretinal deposits called "dots". RPE detachments, retinal pigment epithelial mottling and atrophy together with subretinal fibrin may be reported as well. And finally, in rare cases patients may develop subretinal lipid.
Treatment Options for Central Serous Retinopathy
Fortunately, 80-90% of all cases of central serous retinopathy resolve spontaneously within 3 months. Observation is actually the first step in management of the disease. In case a person is taking corticosteroids he/she should discontinue with these medications (if possible). On the other side, if the person does not take corticosteroids and the condition seems to not get better after two months or the condition has left patient with residual deficit or visual symptoms that interfere in everyday activities the doctor considers active treatment.
There are several treatment modalities for such patients. They include photodynamic therapy and laser coagulation of RPE leakage sites. Furthermore, some medical treatments that have been investigated include Acetazolamide, beta adrenergic receptor blocker propranolol and mixed alpha and beta adrenergic receptor blocker labetalol. And finally, mifepristone, an antagonist of progesterone and glucocorticoid receptors is another drug that has been used in patients suffering from central serous retinopathy.
Your thoughts on this
Loading...