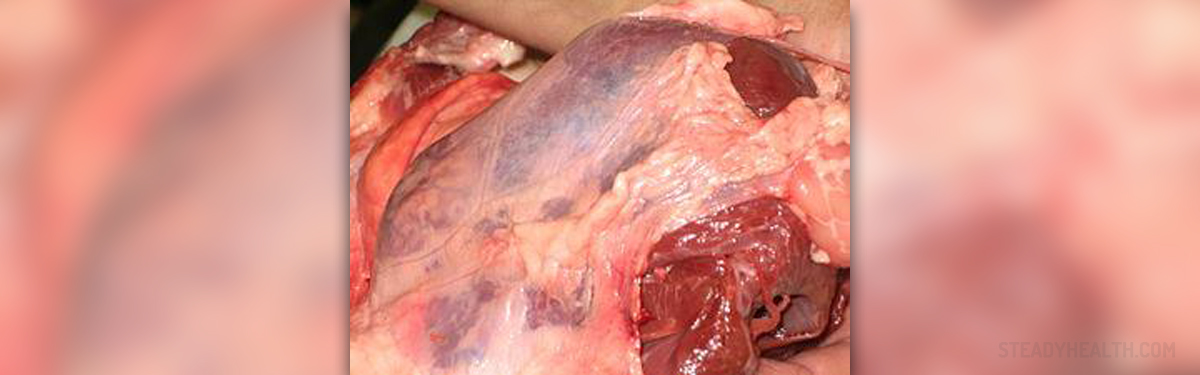
Pericardium is the sac with two layers, surrounding the heart and the roots of great blood vessels, such as vena cavae, aorta, pulmonary veins and pulmonary artery. Its role is to aid cardiac efficiency, anatomically fix the heart though ligamentous connections and to protect the heart form malignancy, infections and some external friction.
Chronic pericarditis is therefore inflammation of the pericardium. As the result of this inflammation, patients suffering from this rare condition usually experience thickening of the pericardium or build up of fluid in pericardial space. Doctors differentiate two main types of pericarditis, chronic effusive and chronic constrictive pericarditis.
About Chronic Effusive Pericarditis (CEP)
In most cases, this condition is idiopathic, meaning it doesn’t have any apparent cause. However, it can be a consequence of acute pericarditis, caused by hypothyroidism, tuberculosis or breast and lung cancers.
Some of the patients are asymptomatic but others complain about dyspnea on physical exertion, chest discomfort or pains, palpitations and lightheadedness. People may also suffer from hiccups, fatigue, cough, hoarseness, confusion and anxiety because of this condition. Additional symptoms may include hypotension, elevated jugular venous pressure (JVP) and diminished heart sounds. In some cases, patients may develop cardiac tamponade as a late complication of this condition.
Patients are usually treated for the cause of CEP. Mild symptoms in patients who are not hemodynamically compromised are usually treated using conservative approach, while other patients may require surgical intervention.
Chronic Constrictive Pericarditis
Causes of chronic constrictive pericarditis (CCP) may involve: viral infections, tuberculosis, some post surgical complications or mediastinal irradiation and in some cases other infections, disorders of connective tissue, drugs, traumas, cardiovascular diseases, uraemia, use of certain drugs and neoplasms. Some chemical traumas and inheritance may also play a role in development of this condition.
Early signs are often too subtle to be noticed. Advanced CCP may be characterized by jaundice, muscle wasting, cachexia, dyspnea, elevated JVP, Kussmaul’s sign, peripheral edema. In some cases, patients suffering from this condition may suffer from pulsatile hepatomegaly, pericardial “knock”, reduced apical impulse and pulsus paradoxus. Intense venous congestion may be followed by some gastrointestinal symptoms.
Medical treatment for CCP patients includes bed rest and the use of diuretic drugs. This and restriction of salt in the diet are known to relieve symptoms of this condition. Although surgical procedure is found to be effective for 85% of the cases, mortality rate is also very high and about 5 to 15% of patients end up with lethal consequences of this surgery.
Your thoughts on this
Loading...