There has been much debate over the years as to the correct place and form of episiotomy. There is a wide variation in the international rate of episiotomy. For example, the rate is 8 per cent in Holland, fourteen per cent in England, fifty per cent in the US and 99% in Eastern Europe. The liberal usage of episiotomy has been opposed by some groups, including the National Childbirth Trust.
Reasons for episiotomy
Episiotomy is often used when delivery is delayed due to rigidity in the perineum. Cutting it might expedite delivery and might prevent a tear. If a tear seems likely, episiotomy might be necessary. In the case of instrumental delivery, including breech delivery, episiotomy might be used. This is because forceps delivery often results in some damage to the perineum. Episiotomy might also be used in the case of a Kielland’s forceps rotation. Premature delivery might be eased slightly by employing episiotomy. This might help to avoid the so-called ‘champagne cork’ effect. Episiotomy should be used in this case even if the baby is small.
Tears of the perineum
Tears of this type are categorized in four ways. First degree tears involve damage to the fourchette and vaginal mucosa, along with exposure of the underlying muscles. Second degree tears apply to the posterior vaginal walls and perennial muscles. In this category, the anal sphincter is intact. Third degree tears involve a tearing of the anal sphincter. However, the vaginal mucosa might be intact. Fourth degree tears refer to an opening of the anal canal and in some cases the rectum.
Performing an episiotomy
An episiotomy is performed in the second stage, normally when the perineum is being stretched. In the case of a forceps delivery, the cut is made after use of the forceps. Local anesthesia might be required in the case of a lack of a good epidural. An existing epidural should be topped up if an episiotomy is going to be performed. Normally, a mediolateral episiotomy is recommended. This type will start at the posterior part of the fourchette. The incisions will then move backwards and turn medially before the border of the anal sphincter. Performance of this type of operation should not be routine. However, there is definitely a legitimate place for the episiotomy procedure in certain cases.
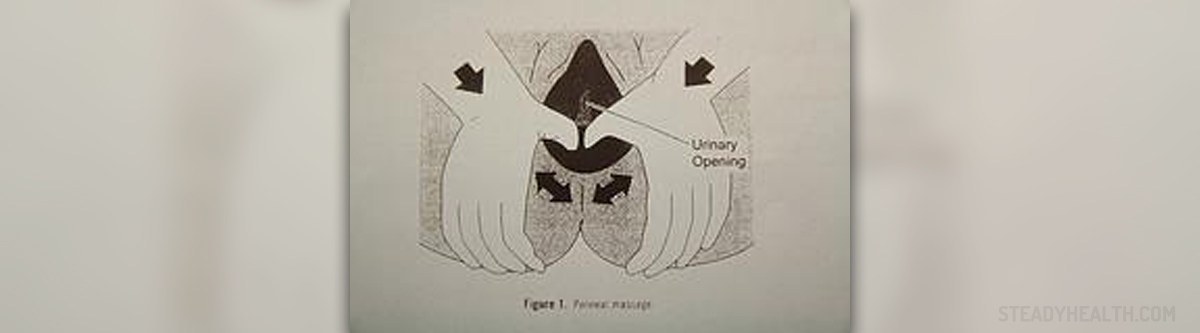
Prevention
Antenatal perineal massage might reduce the likelihood of perineal trauma. However, massage during labor does not seem to be totally effective. Midwives are generally adapted at helping to prevent perineal tears in home deliveries.
Your thoughts on this
Loading...